 Dr. Ed Glaser, DPM
Dr. Ed Glaser, DPM
Dr. Glaser is the President and developer of Sole Supports orthotics.
INTRODUCTION
Previously, the midfoot was modeled as one rigid segment based on the assumption that negligible motion took place within the midfoot (1). We now know that movements including walking and slow running involve considerable motion between midfoot bones (2-4). With this knowledge of midfoot motion it is logical to consider these motions in any attempt to control the foot with an intervention such as a foot orthosis. Perhaps there is evidence that returning the focus to the midfoot, medial longitudinal arch and plantar vault, could yield measurements that relate more to the dynamic gait cycle and result in improved clinical outcomes.
One recent attempt called Foot Posture Index (FPI) was designed to be a valid, simple and clinically useful tool. Its most recent version is based on 6 static foot morphology criteria (talar head palpation, curves above and below the medial malleoli, inversion / eversion of the calcaneus, bulge in the region of the talarnavicular joint, congruence in the medial longitudinal arch, and adduction/abduction of the forefoot on the rearfoot), and although there is some improvement in intrarater reliability and validity with this tool, there continues to exist significant doubt as to its intrerrater reliability (5) and applicability to dynamic function (6).
Another attempt at quantification called the Foot Line Test (FLT) which is a measure of the medial prominence of the navicular in a mediolateral direction, was developed to investigate the relationship between foot morphology and injury development. The measurement of medial/lateral movement of the medial prominence of the navicular is primarily a frontal plane measurement, and so while FLT has been shown to be a reliable measure(7), future work is needed to determine if this measure correlates with dynamic function.
DISCUSSION
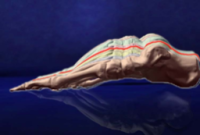
The longitudinal arch angle (LAA) is defined as the angle formed by two vectors – one passing through the midpoint of the medial malleolus to the navicular tuberosity and the other passing through the midpoint of the medial aspect of the first metatarsal head to the navicular tuberosity (fig?). What is interesting about the work done with these angles, is that they are starting to reveal measurements that show good interrater reliability (8), are prognostic of dynamic foot posture during walking and running and may have some value in predicting the risk of lower extremity injuries (9,10). This is good news for the clinician who looks to the published research to confirm and validate his clinical measures.
It seems plausible that the closer the measurements get to a measure of the medial longitudinal arch and plantar vault of the foot, the more applicable they are to the dynamic gait cycle. This correlates with the knowledge that significantly more motion occurs in the sagittal plane during each step of the gait cycle when compared to transverse and frontal motion. Put quite simply, there is an accepted clinical relevance to the arch of the foot and its perceived posture - either low or high - and it may very well be that the closer a measurement gets to describing this posture, the more dynamically relevant it is.
Therefore a distinction is needed between those foot type classifications that focus on frontal plane measurements, and foot posture that is evaluated by the medial longitudinal arch or a three dimensional posture. Looking at some of the more recent measurements that have focused more on the medial longitudinal arch reveals that there has been progress with regards to defining more reliable, clinically relevant measures.
To date, much of the study of foot posture has included discussions of frontal plane orientations such as calcaneal inversion. Given the above mentioned evidence it becomes clear that more clinically relevant measures may be found in the midfoot and medial longitudinal arch. Accounting for the entire plantar vault may give us a better understanding of what changes in foot posture are relevant to our clinical decisions. In an ideal scenario, a measurement would be accurate, reliable, backed by clinical outcomes, describe the entire foot and perhaps most importantly predict the dynamic function of the foot.
So what is the ideal foot posture? The MASS (Maximal Arch Subtalar Stabilization) theory as proposed by Glaser et al(11) is designed to capture the foot in the most corrective posture. It is defined as the maximal amount of closed chain supination that is achievable for any particular foot at midstance, with the heel, first and fifth metatarsals in contact with the ground. The goals of this correction include 1) adequate supination at heel strike, 2) that the forefoot makes full contact on the ground at midstance 3) that the majority of forefoot load is on the first metatarsal joint at heel lift and that 4) the first MPJ is not limited in dorsiflexion. This posture is captured using a gait-referenced sequence with semi-weight-bearing loading. The casting method is the same for all feet though each foot yields a unique three dimensional shape due to unique anatomical variations and flexibility differences. It is based on the concept that if there is a corrected foot posture that is to be achieved, it needs to be emulated and induced directly by the intervention, in this case a foot orthosis. This direct intervention takes the form of a full contact, weight-calibrated, orthosis. Recent investigations have shown that foot orthoses based on this corrected position (or posture) provide relief of lower extremity musculoskeletal pain (12) and improved economy of gait (13).
SUMMARY
Foot posture measurements taken in the MASS posture may prove more applicable to clinical decision making with regards to orthosis manufacture as they can be compared volumetrically to a pronated foot posture or relaxed calcaneal stance position. Knowing that there is an optimal foot posture that may be different for each individual, but based on the same reference points, logic follows that there is a spectrum of function (or dysfunction) and a zone of optimal control. Future writings and investigations will focus on the zones of postural control and their application to treatment with foot orthoses.
References
10. McPoil TG, Cornwall MW. Use of the longitudinal arch angle to predict dynamic foot posture in walking. J Am Podiatr Med Assoc 2005; 95(2):114-120.
11. Glaser E.S., Bursch D, Currie S.J. Theory, Practice Combine for Custom Orthoses. Biomechanics 2006; 13(9):33-43.
12. Trotter LC, Pierrynowski MR. The short-term effectiveness of full-contact custom-made foot orthoses and prefabricated shoe inserts on lower-extremity musculoskeletal pain: a randomized clinical trial. J Am Podiatr Med Assoc 2008; 98(5):357-363.
13. Trotter LC, Pierrynowski MR. Changes in Gait Economy Between Full-Contact Custom-made Foot Orthoses and Prefabricated Inserts in Patients with Musculoskeletal Pain: A Randomized Clinical Trial. J Am Podiatr Med Assoc 2008; 98(6):429-435.