


CBP Chiropractors: We Must Practice What We Teach
 Cindy Boyd, BS, DC
Cindy Boyd, BS, DC
Private Practice of Chiropractic Alameda, CA
Faculty Life Chiropractic College West
&
 Deed E. Harrison, DC
Deed E. Harrison, DC
President CBP Seminars, Inc.
Vice President CBP Non-Profit, Inc.
Chair PCCRP Guidelines
Editor—AJCC
INTRODUCTION
In previous issues of the AJCC, we have presented a number of articles on the indications and contra-indications of the cervical denneroll orthotic device as a method for restoration of an abnormal cervical lordosis. Also, several patient case studies have been presented describing the successful ability of the cervical denneroll orthotic device in restoring the cervical lordosis and improving patient health disorders as a consequence. In the current case, we report on the improvement in the cervical spine with a large disc herniation and complex injury-buckling of the cervical segments including retro-listhesis, hyper-extension, and flexion at different cervical spine joints. This report represents the actual conditions of one of the authors (CB) and these are her results.
Key Case Features
A 34 year old female presented with chronic neck pain, decreased range of motion, headaches with extension of the head and neck and a recent onset of heart palpitations of unknown etiology. The symptoms were reportedly getting worse over the past few months, and causing the patient to refrain from practicing in her chiropractic clinic providing one on one patient care. After administering 1-2 adjustments on any given day, the symptoms were exacerbated causing disability and significant discomfort.
The patient had a past history of two head and neck injuries. The first direct impact injury was sustained during a bicycle accident that occurred in the spring of 2008. The patient was riding a bicycle at a high speed and traversed over old railroad tracks at an awkward angle causing an immediate crash. Her head hit the pavement with significant force, and unfortunately she was not wearing a helmet. Fractures were ruled out and no lacerations were present. A mild concussion was sustained. Bruising and swelling was present in the right zygomatic region at the site of direct impact.
Two years later, a double direct impact injury occurred during a snowboarding accident where the patient fell on an ice patch directly landing on the sacrum and a second impact occurred during the same fall when she fell backwards and hit her skull on the ice patch with significant force. This time the patient was wearing a helmet.
- · Health Status, Pain, and Disability Questionnaires
The short form (Sf)-36 health status questionnaire, numerical rating scale for pain intensity and the neck disability questionnaires were administered. The patient had considerable pain, disability, and depressed health. See Figure 1 for the initial NDI and SF-36 abnormalities.
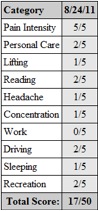
 Figure 1. Patient initial neck disability and SF-36 scores indicating considerable pain, disability, and abnormal health status.
Figure 1. Patient initial neck disability and SF-36 scores indicating considerable pain, disability, and abnormal health status.
- Radiographic Evaluation
Lateral Cervical Radiograph:
On 8/24/11 a digital lateral cervical was obtained. See Figure 2. The radiographic analysis was done using the Posture RayÒ computerized radiographic mensuration system. The patient’s radiographic displacement values are shown in Figure 2B and are compared against normal. Several cervical spine subluxation-displacements are present including: an abnormal kyphosis from C4-C7, a C3-C4 segmental retro-listhesis, and a considerable hyper-extension of C2-C3 were identified. The radiographic and clinical findings indicated a possibility of herniation one or more cervical discs and instability in multiple levels of the cervical spine. Thus, an MRI was obtained, and the findings confirmed a central/sub-ligamentous disc herniation at C2/C3 and C5/C6 with concomitant instability.

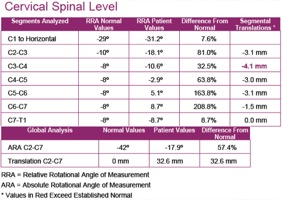 Figure 2. Initial lateral cervical radiograph and abnormal findings of alignment compared to ideal values. The PostureRay™ system was used.
Figure 2. Initial lateral cervical radiograph and abnormal findings of alignment compared to ideal values. The PostureRay™ system was used.
Lateral Thoracic Radiograph:
On 8/24/11 a lateral thoracic radiograph was also obtained. Figure 3 depicts the patient's lateral thoracic radiograph. Relative to the CBP ideal thoracic elliptical model, the patient's upper and mid-thoracic segments are in a relative subluxated extension position. This is consistent with an extension abnormal postural position of the thorax relative to the pelvis or lumbar spine.
 Figure 3. Lateral thoracic radiograph. The green elliptical line is the Harrison ideal thoracic model representing the proper path of the posterior vertebral bodies of the thoracic spine. Note that the patient has extension-backwards bending of the upper-mid thoracic spine relative to the lower thoracic spine.
Figure 3. Lateral thoracic radiograph. The green elliptical line is the Harrison ideal thoracic model representing the proper path of the posterior vertebral bodies of the thoracic spine. Note that the patient has extension-backwards bending of the upper-mid thoracic spine relative to the lower thoracic spine.
Denneroll Stress Radiography:
These values and findings indicate the patient’s candidacy for the Denneroll Cervical Orthotic. Based on MRI findings and significant abnormal segmental cervical translation measurements, Denneroll stress X-rays were taken using the large cervical Denneroll. Figure 4 depicts the lateral stress x-ray. Based on the initial radiographs, it was determined additional upper thoracic flexion and translation was needed in this setup to make a considerable correction in the injured and postural distorted regions. Thus, a 10 millimeter foam block was used under the denneroll device to increase the height of the orthotic in order to induce additional upper thoracic flexion and translation during the stress study. The peak of the denneroll was placed in the lower cervical spine. Particular attention was given to the hyperextended upper cervical segments, and another block measuring 10 millimeters in height was placed under base of the skull during the stress analysis. Further, to limit the amount of skull extension and upper cervical extension, the patient was asked to actively flex-tuck her chin (although painful) at the time the radiograph was taken. Figure 2 shows the upper cervical spine extension on the initial patient x-ray.
The stress analysis study showed considerable correction in the cervical abnormal values including the segmental translations and relative rotation angles that were present on the neutral lateral cervical study.

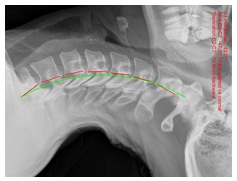 Figure 4. Denneroll stress lateral thoracic radiograph to ensure proper location of the denneroll peak and if the denneroll is effectively improving the cervical alignment.
Figure 4. Denneroll stress lateral thoracic radiograph to ensure proper location of the denneroll peak and if the denneroll is effectively improving the cervical alignment.
- Denneroll Cervical Orthotic Intervention
Based on the outcomes of the stress radiographic analysis, the patient agreed to participate in a study to determine the outcome of cervical curve correction using the Denneroll home traction device. No other forms of treatment were administered. Spinal manipulation, CBPÒ drop table adjustments, Mirror ImageÒ exercises and in office traction types, were all avoided during this particular patient treatment phase with the Denneroll.
The large cervical Denneroll was used at a frequency of 1-2 times daily, 4-6 days a week for a 30 day period. Each home session involved the patient lying supine on the large cervical Denneroll with a 10 millimeter block under the device. Refer to Figure 4 for the denneroll setup. In addition, a 10 millimeter block was placed under the skull to limit the amount of upper cervical extension. The patient was also instructed to actively flex the chin while on the device. The amount of upper cervical hyperextension and thoracic extension measured on the lateral cervical and thoracic radiographs warranted the degree of specificity in this setup. Between the dates of 8/24/11-9/22/11 approximately 36 home Denneroll sessions were performed at a duration of 10-18 minutes each.
A follow up lateral cervical x-ray was taken on 9/22/11 to determine if the intervention had made any significant changes.
- Case Outcome
Subjectively, at the end of the 1-month treatment phase, the patient was asymptomatic including the disappearance of the heart palpitations, headaches and pain. There were significant improvements in the SF-36 and neck disability outcomes. The follow up lateral cervical radiograph exam showed significant improvements in all cervical regions that were abnormal initial. Figure 5 and Table 1 describe these results.
 Figure 5. One-month follow-up lateral cervical. Note that this x-ray was taken a minimum of one day with no treatment interventions. There are considerable improvements in all radiographic abnormalities.
Figure 5. One-month follow-up lateral cervical. Note that this x-ray was taken a minimum of one day with no treatment interventions. There are considerable improvements in all radiographic abnormalities.
|
RRA’s (-) values = extension (+) = flexion |
Segmental Translation (-) values = posterior |
Translation C2-C7 |
|
|
C2/C3 |
12° |
-1.6 mm |
21.6mm |
|
C3/C4 |
-1.7° |
-2.4mm |
|
|
C5/C6 |
0° |
-0.8 mm |
|
|
ARA C2-C7 |
-26° |
|
|
CONCLUSION
This case report represents the actual conditions of one of the current study authors (C.B.). The uniqueness of this case lies in the severity of the cervical spinal displacements and the concomitant improvements in structural and functional abnormalities using the cervical Denneroll as the exclusive treatment intervention. While the patient's follow-up radiograph is still not considered to be within normal limits and further care is warranted, the improvements over the course of one-month are promising. The patient (C.B.) has committed to continuing her Denneroll intervention program to continue rehabilitating her cervical spine. Afterall, as a CBP Chiropractor, we must practice for ourselves what we teach our patients to do.
 CBP Seminars
CBP Seminars